Hormonal Optimisation: The Complete Science of Engineering Your Endocrine System for Peak Strength, Drive, and Longevity
You cannot supplement your way to hormonal balance. Testosterone, cortisol, thyroid, growth hormone, and insulin form a signalling cascade — and you can’t fix a cascade from the bottom.
The endocrine cascade mapped alongside mapped below shows why every axis must be addressed from the hypothalamus down.
Five hormones cascade from one control centre — one axis out and the whole system compensates.
Hormonal optimisation is the process of keeping your body’s chemical messengers balanced and performing at their best. Five hormone systems control your drive, stress response, metabolism, tissue repair, and how your body uses food. They all flow from two master glands in your brain — and when one system falls out of rhythm, the others compensate by degrading. Getting the upstream signals right fixes downstream problems.
Testosterone — The Drive Axis
The HPG axis governs motivation, muscle synthesis, and cognitive drive. Declining testosterone signals that upstream inputs are degrading.
Cortisol — The Stress Axis
Acute cortisol enhances performance. Chronic cortisol suppresses testosterone, thyroid, and immunity. The HPA axis doesn’t need silencing — it needs rhythm.
Thyroid — The Metabolic Engine
T3 and T4 set the metabolic rate for every cell. Subclinical hypothyroidism — too subtle for standard bloodwork — silently caps energy and cognition.
Growth Hormone — The Repair Axis
GH pulses during deep sleep to drive tissue repair, fat metabolism, and immunity. Disrupted sleep architecture shuts down the repair factory.
Insulin — The Partitioning Switch
Insulin decides whether calories become muscle glycogen or visceral fat. Sensitivity isn’t a diabetes metric — it’s the gatekeeper of nutrient partitioning.
TLDR: 10 Hormonal Tactics. 10 Endocrine Myths Busted.
Everything below distilled into 20 cards. Deploy the tactics, debunk the myths. The full science follows after.
Hormonal Optimization
Why Hormones
Control Everything
Hormones aren’t isolated chemicals—they’re an integrated signaling network that determines your physical capacity, cognitive performance, metabolic efficiency, emotional state, and rate of aging.
You already know hormones matter. You’ve heard about testosterone for muscle building, cortisol for stress, maybe insulin for blood sugar. But here’s what the fitness and biohacking industries systematically miss: hormones are the operating system on which all performance software runs.
The Performance Gap: You can have perfect training programming, optimal nutrition, and adequate sleep—and still perform at 60% capacity if your hormones are suboptimal. Conversely, optimized hormones amplify every other intervention.
The Mortality Link: Men with testosterone levels in the lowest quartile (<300 ng/dL) have an 88% higher cardiovascular mortality risk compared to the highest quartile. Optimization isn't just about performance; it's about survival. Even within the "normal" range, the difference between 400 ng/dL and 700 ng/dL is profound.
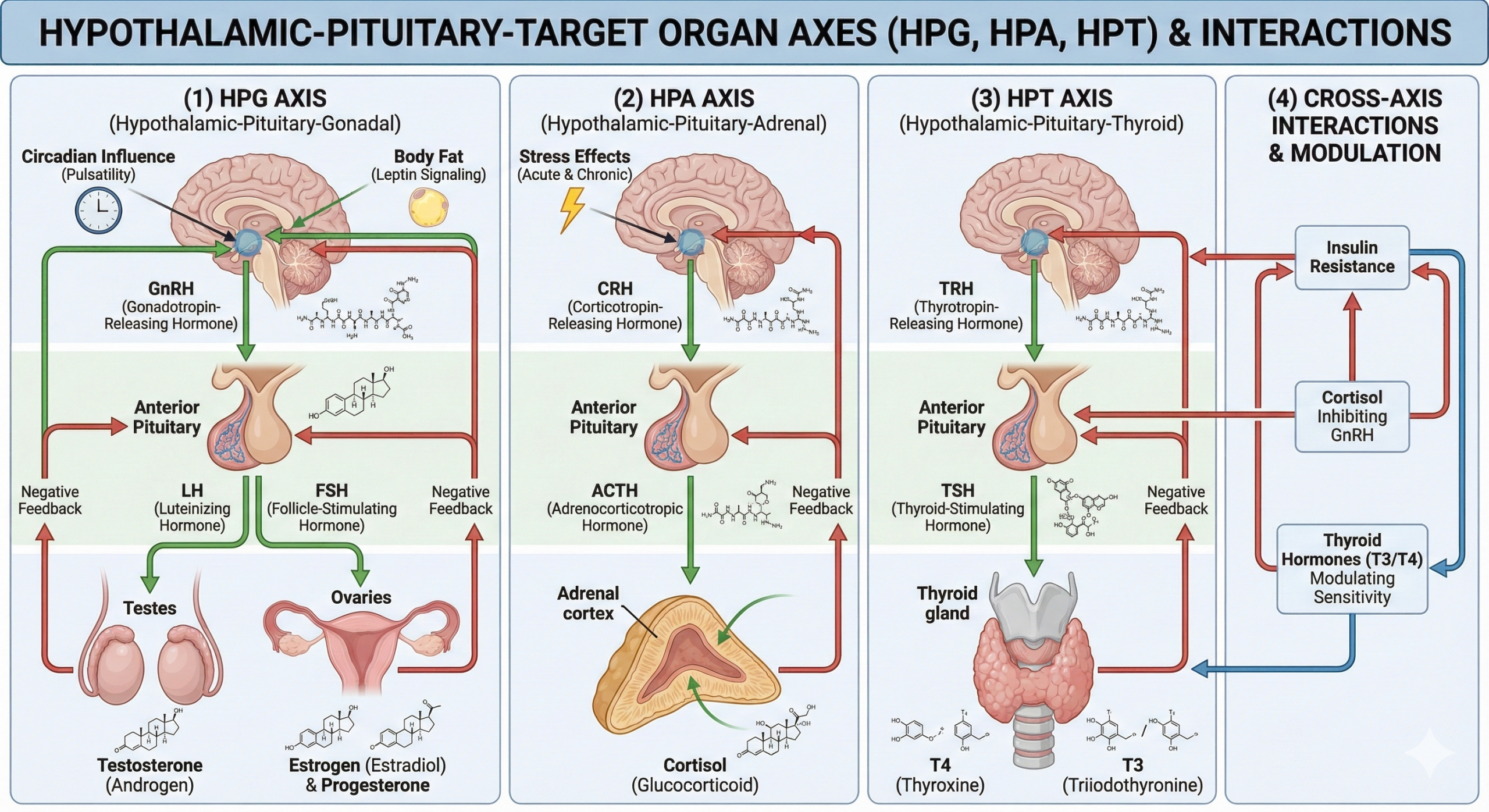
The Integrated Network
Your hormones exist in dynamic equilibrium with feedback loops, synergies, and antagonisms.
The Age Factor: Decline Is Not Destiny
Hormonal decline with aging is real but highly variable. Biology loads the gun; lifestyle pulls the trigger.
The Endocrine Disruptor Crisis
Modern environments contain thousands of synthetic chemicals that disrupt endocrine function. Reducing exposure can increase testosterone by 10-20%.
Xenoestrogens
Found in BPA (plastics, receipts) and Parabens (cosmetics). They bind to hormone receptors and disrupt synthesis.
Anti-Androgens
Found in Phthalates (soft plastics, lotions) and certain pesticides. Directly reduce testosterone production.
High-Leverage Mitigation
Use glass/stainless steel for food storage (never microwave plastic). Filter drinking water. Avoid thermal receipts. Use cast iron cookware.
Hormonal optimization isn’t about boosting testosterone, it’s about optimizing your Integrated Endocrine System.
Testosterone: Foundation of
Strength & Drive
Testosterone is the most extensively studied performance hormone, and for good reason: it’s the primary determinant of muscle mass, strength, bone density, and libido in men—and remains important for these functions in women at lower concentrations.
Understanding the Measurements
-
1. Total Testosterone
All testosterone in blood (both bound and unbound).
Reference ranges: Men 300-1000 ng/dL, Women 15-70 ng/dL
This is the most commonly measured but least informative metric. -
2. Free Testosterone
Testosterone not bound to proteins (~2-3% of total). Biologically active, can enter cells and bind to androgen receptors. Better predictor of androgenic effects than total testosterone.
Reference ranges: Men 50-200 pg/mL, Women 1.0-8.5 pg/mL -
3. Bioavailable Testosterone
Free testosterone + testosterone loosely bound to albumin (~40-50% of total). Can dissociate from albumin and become active. The most accurate measure of functional testosterone.
Sex hormone binding globulin (SHBG) binds testosterone tightly, making it unavailable. Approximately 60-70% of testosterone is bound to SHBG (inactive).
SHBG Increases With:
- Aging (reduces free T even if total remains stable)
- Hyperinsulinemia (chronic insulin resistance)
- Hyperthyroidism or excess thyroid hormone
- Low growth hormone/IGF-1
- Certain medications (estrogen increasing)
SHBG Decreases With:
- Obesity (initially—very low SHBG in obesity)
- Hypothyroidism
- Growth hormone or IGF-1 excess
- Anabolic steroid use
The Production Pathway
- Step 1: Hypothalamus — GnRH (gonadotropin-releasing hormone) released in pulsatile fashion. Regulated by: leptin (energy availability), stress (cortisol inhibits), and sleep (peaks during sleep).
- Step 2: Pituitary — LH (luteinizing hormone) and FSH released. LH stimulates Leydig cells in testes to produce testosterone; FSH stimulates spermatogenesis.
- Step 3: Testes (Leydig Cells) — Cholesterol converted to testosterone through enzyme cascade. Requires: cholesterol availability, zinc, magnesium, vitamin D as cofactors. Produces ~95% of testosterone in men.
- Step 4: Peripheral Conversion — Some T converted to estradiol by aromatase (in fat/liver). Some converted to DHT by 5-alpha-reductase. Balance between testosterone, estrogen, and DHT matters for optimal function.
- Negative Feedback: High testosterone inhibits GnRH and LH. This maintains homeostasis and explains why exogenous testosterone (TRT) suppresses natural production.
Factors That Optimize Production
Acute Effects: Heavy resistance training (>70% 1RM) acutely increases testosterone by 15-40% for 30-60 minutes post-workout. Large muscle groups (squats, deadlifts) produce greater response.
Chronic Adaptations: Regular training increases baseline T by 15-25% and increases androgen receptor density. Trained older men often have levels similar to sedentary younger men.
Optimal Protocol
- Frequency: 3-4 sessions weekly.
- Volume: 3-6 exercises per session, 3-5 sets each.
- Intensity: 70-85% 1RM, 6-12 reps (strength-hypertrophy range).
- Movements: Compound movements prioritized (squats, deadlifts, presses).
- Rest: 60-120 seconds (balances mechanical tension and metabolic stress).
Warning: Excessive volume/intensity without recovery suppresses testosterone. Monitor via HRV.
70% of daily testosterone secretion occurs during REM and slow-wave sleep. Sleep quality matters as much as quantity.
- One week of 5-hour sleep reduces testosterone by 10-15%.
- Chronic sleep restriction (<6 hours nightly) reduces testosterone by 10-20% baseline.
- Each hour of sleep loss correlates with ~10-15% testosterone reduction.
- Optimization: 7-9 hours duration. Consistent sleep/wake schedule (circadian entrainment). Maximize deep sleep.
Adipose tissue (especially visceral fat) contains high concentrations of aromatase enzyme, which converts testosterone → estradiol (estrogen).
- The Cycle: More body fat = more aromatase = lower testosterone / higher estrogen. Estrogen provides negative feedback to hypothalamus, further suppressing T.
- Impact: BMI >30 correlates with testosterone 150-200 ng/dL lower than lean individuals. Each 5-point BMI increase drops T by ~50 ng/dL.
- The Fix: 10% body weight reduction increases T by 50-100 ng/dL.
- Optimal Range: Men 10-15% body fat, Women 18-25%.
Cortisol directly inhibits GnRH production in the hypothalamus and inhibits LH action on Leydig cells. Chronic stress (sustained cortisol) reduces testosterone by 20-40%.
Optimization: Daily meditation (reduces cortisol 15-30%), strategic deload weeks (every 4-6 weeks), and prioritizing recovery. T:C ratio (Testosterone to Cortisol) predicts recovery capacity.
Macronutrients
- Calories: Chronic restriction (>25% deficit) suppresses T by 15-30%. Cycling deficits prevents suppression.
- Fats: Low-fat diets (<20%) suppress T by 10-20%. Target 25-35% of calories. Include saturated fat (cholesterol precursor) and monounsaturated (olive oil, avocado).
- Protein: 1.6-2.2 g/kg bodyweight. Very high protein (>3.0g) without adequate fat/carbs may reduce T.
- Carbs: Very low-carb (<50g) may suppress T acutely. Carb cycling supports training demand.
Critical Micronutrients
- Vitamin D: Receptor in Leydig cells. Deficiency (<30 ng/mL) correlates with low T. Target 40-60 ng/mL.
- Zinc: Cofactor for synthesis. Deficiency common in athletes due to sweat loss. Dose: 15-30 mg daily (balance with copper).
- Magnesium: Reduces SHBG, increasing free T. Dose: 300-500 mg daily.
- Boron: Emerging evidence for lowering SHBG (increasing free T by 25%). Dose: 6-10 mg daily.
Reducing exposure to xenoestrogens can increase testosterone by 10-20% in high-exposure individuals.
- Eliminate plastic food storage (use glass/stainless steel).
- Refuse thermal receipts (BPA coating).
- Filter drinking water (remove atrazine, perchlorate, PFAS).
- Choose organic for “dirty dozen” produce.
- Use clean personal care products (avoid phthalates, parabens).
- Avoid non-stick cookware (PFAS exposure).
Testosterone optimization is primarily Lifestyle-Mediated, not supplement dependent.
The Cortisol Axis:
Master Performance Regulator
Cortisol has been demonized as “the stress hormone” to be minimized. This is profoundly wrong. Cortisol is essential for survival, performance, and health. The goal isn’t low cortisol—it’s optimally regulated cortisol with robust acute responses and proper circadian rhythm.
The Glucocorticoid Master Key
1. Metabolic Regulation
Increases blood glucose (gluconeogenesis), mobilizes amino acids, and promotes lipolysis (fat breakdown). It provides the fuel for fasting, exercise, and acute stress.
2. Immune Modulation
Anti-inflammatory at physiological levels. It suppresses excessive immune activation, prevents autoimmune responses, and balances Th1/Th2 response.
3. Cognitive Enhancement
Enhances memory consolidation for emotionally salient events and supports executive function and decision-making under pressure.
4. Permissive Effects
Allows other hormones to function. Without adequate cortisol, catecholamines and thyroid hormones fail to exert their full effects.
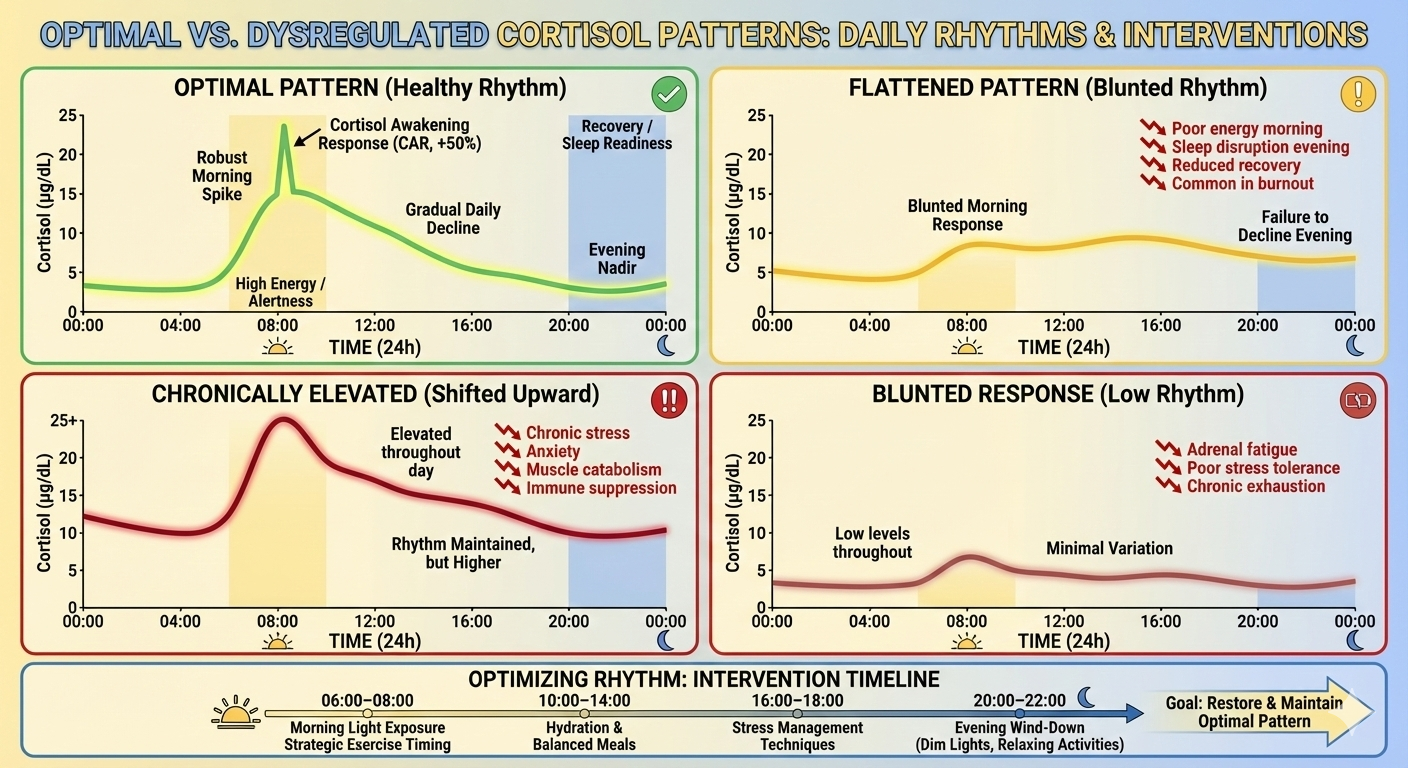
The Cortisol Rhythm: Timing Is Everything
-
Cortisol Awakening Response (CAR):
A sharp spike (50-75% increase) within 30 minutes of waking. This prepares the body for the day’s demands. A healthy CAR indicates robust HPA axis function. -
Morning Peak (30-60 min post-waking):
Typical range: 10-25 μg/dL. Provides energy, alertness, and metabolic activation. -
Gradual Decline:
Steady decrease through the day. By evening (6-8 PM), levels should be 50-60% lower than the morning peak. -
Evening Nadir (10-11 PM):
Lowest levels (2-5 μg/dL). Low cortisol is required for melatonin rise, growth hormone release, and sleep initiation.
Morning too low, evening too high. Results in morning fatigue (“tired but wired”) and evening insomnia. Common in burnout and chronic fatigue.
High baseline all day. Results in anxiety, muscle catabolism, and immune suppression. Driven by acute severe stress or anxiety disorders.
Optimizing Cortisol: Rhythm, Not Suppression
Morning Protocol
- Light: 10-30 mins bright light (ideally outdoor) within 30-60 mins of waking. Blue wavelengths trigger the CAR.
- Activity: Physical movement reinforces the morning peak.
Evening Protocol
- Light Restriction: Reduce bright/blue light 2-3 hours before bed to allow natural cortisol decline.
- Effect: Facilitates melatonin rise and recovery processes.
Exercise creates an adaptive acute cortisol spike. Timing matters.
Capitalizes on high morning cortisol. Reinforces the awakening response and circadian rhythm.
Ideal for performance (body temp peak). Acute spike followed by evening decline.
Can delay cortisol decline and impair sleep onset in sensitive individuals. Monitor sleep quality.
- Avoid Chronic Low-Carb: Very low carb (<50g) can elevate cortisol chronically via gluconeogenesis demand. Carb cycling (higher around training) mitigates this.
- Caloric Sufficiency: Chronic severe restriction elevates cortisol (starvation signal). Moderate deficits (10-20%) are safer.
- Caffeine: Acutely spikes cortisol. Use in AM to reinforce rhythm. Avoid after 2 PM to protect evening decline.
- Anti-Inflammatory: Omega-3s (2-3g EPA/DHA) and Polyphenols reduce inflammation-driven cortisol elevation.
Psychological stress is the primary driver of HPA axis dysregulation.
Evidence-Based Tools
- Meditation: 20 mins daily reduces cortisol 15-30%.
- Breathing: Slow breathing (5-6 breaths/min) activates parasympathetic tone.
- Nature: 20 mins “forest bathing” reduces cortisol 15-25%.
Cognitive Reframing
Perception of control matters more than the stressor. Reframing a “threat” as a “challenge” reduces the physiological cortisol response by 20-40%.
5. Targeted Supplementation
Reduces cortisol 15-30%. Improves resilience.
Dose: 300-500mg (5% withanolides).
Reduces fatigue, modulates stress response.
Dose: 200-600mg (3% rosavins).
Blunts exercise-induced cortisol. Good for high training volume.
Dose: 400-800mg.
Promotes relaxation without sedation. Synergistic with caffeine.
Dose: 200-400mg.
Cortisol is not the enemy, Dysregulation is the problem.
The Thyroid Axis:
Metabolic Master Regulator
Thyroid hormones regulate metabolic rate, energy production, and body temperature. Subclinical hypothyroidism (even within “normal” ranges) profoundly impairs performance.
Understanding the Hormones
-
TSH (Thyroid Stimulating Hormone)
Released by the pituitary. Inverse relationship: High TSH = Hypothyroid.
Optimal Range: 0.5-2.5 mIU/L. (Lab range often 0.4-4.5) -
T4 (Thyroxine)
The primary output (80-90%). Relatively inactive “storage” hormone.
Optimal Free T4: Mid-to-upper range (1.2-1.6 ng/dL). -
T3 (Triiodothyronine)
The active hormone (3-4x more potent). 80% is converted from T4 in the liver/gut.
Optimal Free T3: Mid-to-upper range (3.0-4.0 pg/mL). -
Reverse T3 (rT3)
Inactive “metabolic brake” produced during stress/illness. Competes with T3.
Optimal: <15 ng/dL.
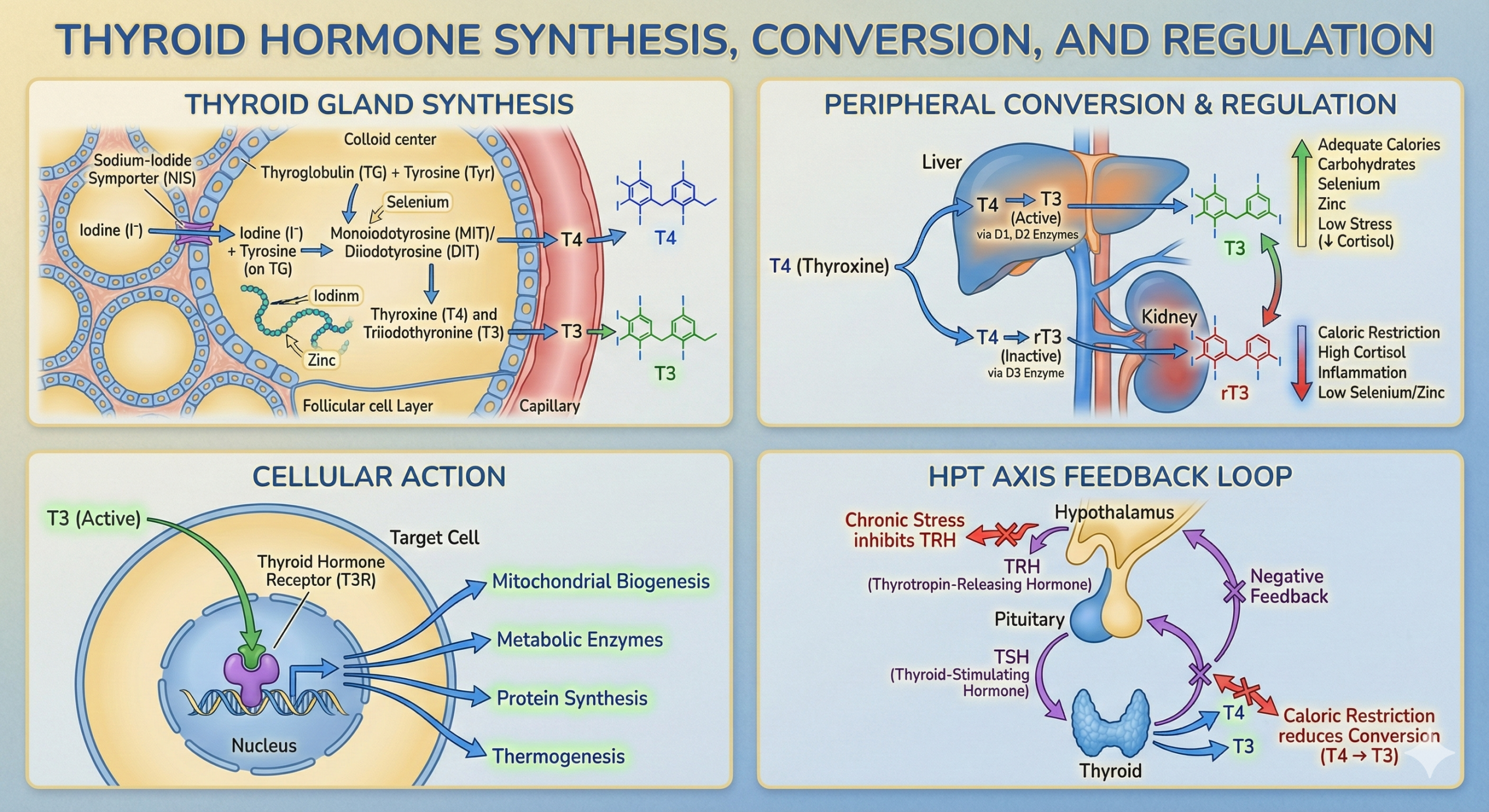
The Conversion Problem
Your thyroid may produce enough T4, but if you cannot convert it to active T3, you remain hypothyroid at the cellular level.
Factors Affecting Function
Metabolic Adaptation
Chronic caloric restriction reduces T3 by 15-30% via adaptive thermogenesis. Low leptin signals energy scarcity → Reduced TSH → Lower T4 output.
Optimization: Avoid deficits >25%. Include diet breaks/refeeds every 2-4 weeks.
Low-Carb Impact
Very low carb (<50g) suppresses T3 by 10-20% because insulin is required for the deiodinase enzyme (T4→T3 conversion).
Optimization: Cycle carbs higher on training days. Maintain 100-150g baseline for most.
2. Critical Nutrient Cofactors
Thyroid synthesis is nutrient-expensive. Deficiencies act as rate-limiters.
Essential building block (T4 has 4 iodine atoms).
Optimal: 150-300 μg daily (Seafood, Salt).
Required for T4→T3 conversion and protection from oxidative damage.
Dose: 100-200 μg (Brazil nuts).
Required for TRH synthesis and T4→T3 conversion.
Dose: 15-30 mg (Balance with Copper).
Required for thyroid peroxidase enzyme.
Optimal Ferritin: >50-70 ng/mL.
Chronic stress suppresses thyroid function via multiple pathways:
- Cortisol inhibits TSH secretion.
- Cortisol inhibits T4 → T3 conversion.
- Cortisol increases T4 → Reverse T3 (inactive).
Clinical Pattern: TSH normal, Free T3 low, Reverse T3 elevated. Diagnosis: Stress-induced hypothyroidism.
Sleep & Body Comp
- Sleep: Deprivation suppresses TSH. 7-9 hours required.
- Fat Mass: Severe obesity impairs function (Leptin resistance). Extreme leanness (<6%) suppresses thyroid (Starvation signal).
Endocrine Disruptors
- Perchlorate/PFAS: Inhibit iodine uptake. Filter water (RO).
- BPA/Phthalates: Disrupt receptor binding. Avoid plastics.
- Testing: Don’t rely on TSH alone. Full panel: TSH, Free T4, Free T3, Reverse T3, TPO Antibodies.
- Nutrition: Adequate calories (maintenance periods), sufficient carbs (>100g), and nutrient density (Se, Zn, I).
- Stress: Cortisol management is thyroid management. Meditation and adaptogens (Ashwagandha 300-500mg).
- Medical: If TSH >4.5 or symptomatic, T4/T3 therapy may be indicated under supervision.
Thyroid function is far more nuanced than TSH Screening suggests.
The Growth Hormone Axis:
Recovery & Regeneration
Growth hormone (GH) and its downstream mediator IGF-1 are critical for muscle growth, fat loss, bone density, tissue repair, cognitive function, and longevity.
Understanding the GH/IGF-1 System
Growth Hormone (GH)
Peptide hormone secreted by the anterior pituitary in discrete pulses (not constant). It has a short half-life (20-30 mins) and drives lipolysis (fat loss) and glucose metabolism directly.
IGF-1 (Insulin-Like Growth Factor)
Produced primarily in the liver in response to GH. It has a long half-life (12-15 hours) and mediates most anabolic effects: muscle protein synthesis, bone growth, and neuroprotection.
The Pulsatile Secretion Pattern
GH is released in 6-10 discrete pulses per 24 hours. The largest pulse occurs 60-90 minutes after sleep onset (during slow-wave sleep).
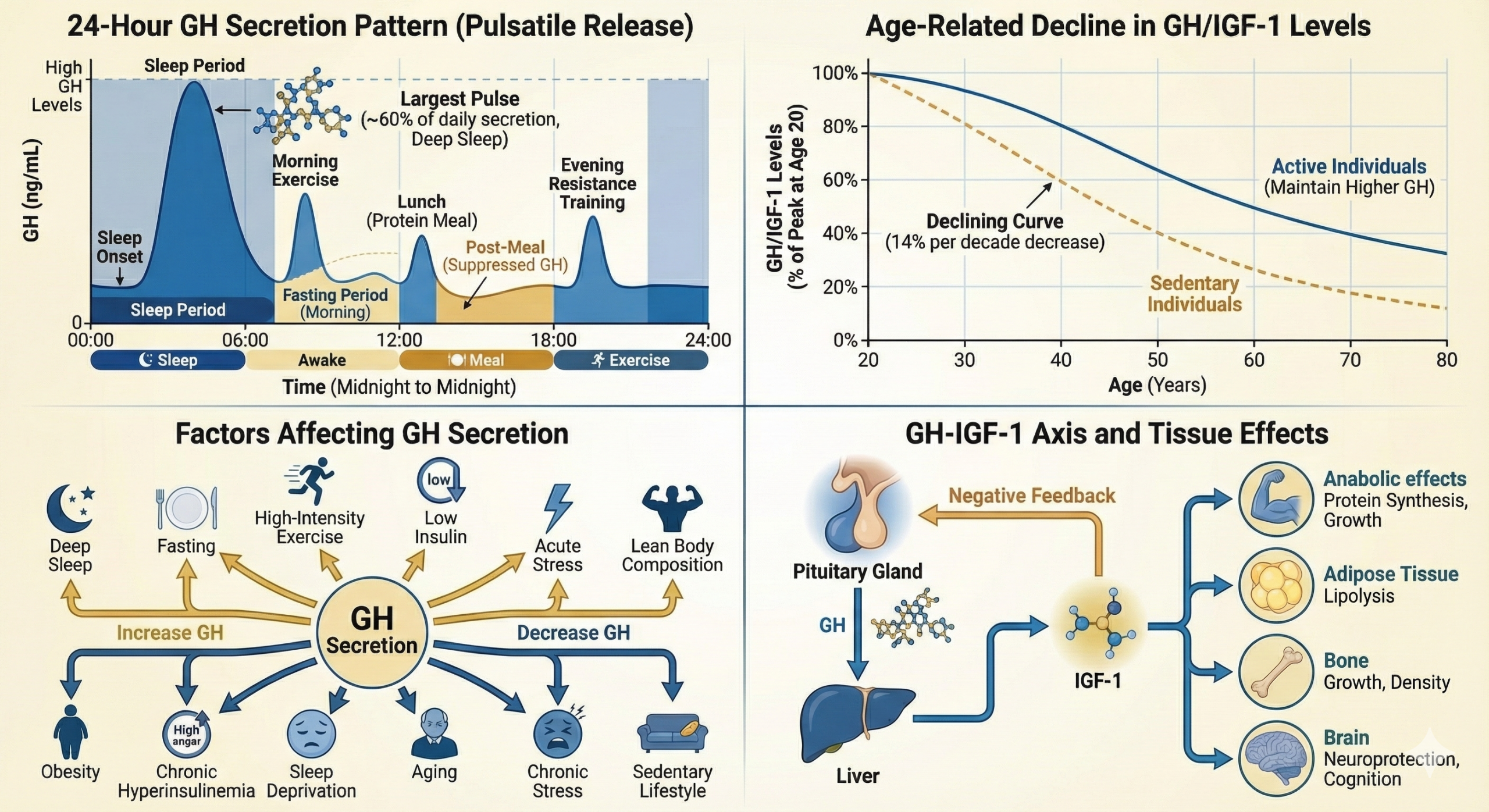
Factors Increasing GH
- Deep sleep (Slow-Wave Sleep)
- Fasting (especially >12-16 hours)
- Exercise (High-Intensity/HIIT)
- Low Insulin (Counter-regulatory)
- Acute Stress
Factors Decreasing GH
- Aging (14% decline per decade)
- Obesity (Inverse correlation)
- Chronic Hyperinsulinemia
- Sleep Deprivation
- Chronic Stress (Cortisol)
GH secretion declines ~14% per decade after age 20. By age 60, secretion is 70-80% lower than peak.
- Consequences: Sarcopenia (muscle loss), visceral fat gain, bone density loss, thinner skin, and cognitive decline.
- The Paradox: While lower GH correlates with longevity in some studies (less growth signaling = less cancer risk), optimal healthspan requires maintaining pulsatile secretion without chronic elevation.
Natural Optimization Protocols
70-80% of daily GH secretion occurs during sleep, specifically during the first deep sleep cycle (Stage 3 Slow-Wave Sleep).
- The Risk: One night of sleep deprivation reduces GH secretion by 70-80%. Sleep fragmentation eliminates the major pulse.
- Optimization: 7-9 hours nightly. Maximize deep sleep via temperature control and darkness.
Fasting increases GH by 300-500% to maintain muscle mass and mobilize fat. Low insulin permits GH secretion.
Mechanism
24-hour fasts increase GH 5-fold in men. Even 12-16 hour overnight fasts provide significant increases via elevated free fatty acids.
Practical Application
16:8 Protocol (16h fast / 8h feed). Caution: Extended fasting >24h repeatedly can suppress thyroid and testosterone.
Heavy loads (70-85% 1RM) create acute GH spikes of 200-500%. Short rest periods (60-90s) maximize metabolic stress (Lactate).
Max effort sprints (30s on / 90s off) trigger robust GH release. 15-25 minutes total duration is sufficient.
4. Nutrition & Supplementation
Focus on avoiding hyperinsulinemia and utilizing specific amino acids.
- Protein Timing: Pre-sleep casein (30-40g) sustains amino acid availability during the sleep GH pulse.
- Insulin Control: Chronically elevated insulin suppresses GH. Avoid snacking and high glycemic loads before bed.
- Arginine/Ornithine: Large doses (5-10g) required. Results inconsistent (30-100% increase possible).
- Glycine: 3g before bed may increase GH via sleep improvement.
- GABA: 3-5g dose shows some evidence for GH increase.
Verdict: Supplements provide 20-40% increases. Lifestyle (Sleep/Fasting/Exercise) provides 200-500% increases. Focus on the foundation.
Growth Hormone optimization is driven by Physiological Spikes, not supplements.
The Insulin Axis:
Metabolic Efficiency
Insulin is essential for nutrient storage, muscle growth, and recovery. The problem isn’t insulin—it’s chronic hyperinsulinemia and insulin resistance.
Understanding Insulin
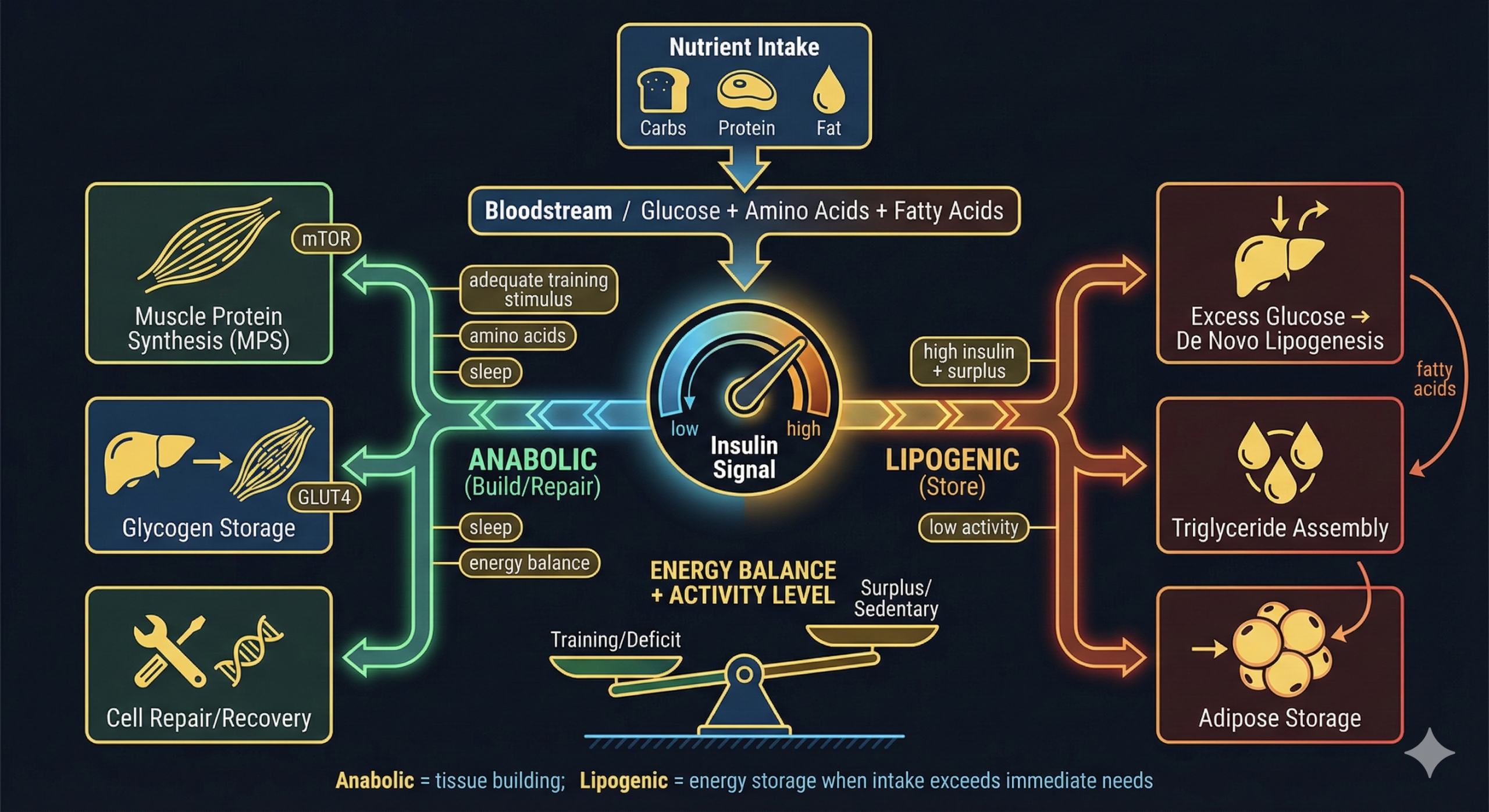
Primary Functions
- Glucose Regulation: Lowers blood glucose by promoting uptake into cells. Stimulates glycogen synthesis.
- Anabolic Effects: Stimulates muscle protein synthesis (mTOR pathway) and amino acid uptake.
- Fat Storage: Promotes lipogenesis (fat synthesis) and inhibits lipolysis (fat breakdown).
The Goal
High Sensitivity + Strategic Timing.
You want a strong response to small amounts of insulin, with spikes restricted to post-training windows, and low baselines at all other times.
Sensitivity vs. Resistance
Optimal Sensitivity
- Fasting Insulin: <5 μIU/mL (Excellent)
- Fasting Glucose: <90 mg/dL
- HbA1c: <5.4%
- HOMA-IR: <1.0
Insulin Resistance
- Fasting Insulin: >10-15 μIU/mL
- Consequences: Fat storage, muscle loss (anabolic resistance), suppressed testosterone, cognitive decline.
Optimizing Insulin Sensitivity
Muscle accounts for ~80% of glucose disposal. Resistance training increases GLUT4 transporters independent of insulin.
- Acute Effect: A single session improves insulin sensitivity by 20-50% for 24-48 hours.
- Chronic Effect: Regular training improves baseline sensitivity by 30-50%.
- Optimization: 3-4 sessions/week. Focus on large muscle groups (Legs, Back, Chest).
Post-Workout Window: Insulin sensitivity is 3-5x higher. Glucose is preferentially stored as glycogen, not fat.
- Protocol: Consume 30-50% of daily carbs within 2 hours post-training.
- Avoid: Constant snacking. 2-3 meals/day allows insulin to return to baseline.
The Virtuous Cycle: Fat loss improves insulin sensitivity, which makes further fat loss easier.
- Impact: 10% weight loss = 30-50% improvement in sensitivity.
- Target: Men 10-15% body fat, Women 18-25%.
Sleep Deprivation: A single night of poor sleep reduces insulin sensitivity by 20-30%. Chronic restriction (<6h) reduces it by 30-40%.
Circadian Timing: Glucose tolerance naturally declines in the evening. Late-night eating creates a larger insulin response than the same meal eaten earlier.
Dietary Levers
- Fiber: 30-40g daily. Slows absorption.
- Protein: 1.6-2.2 g/kg. Combined with carbs, it reduces the glucose spike.
- Vinegar: 1-2 tbsp before meals reduces post-meal glucose by 20-30%.
- Cinnamon: 1-6g daily improves sensitivity via signaling pathways.
Targeted Supplements
- Berberine: 500mg, 2-3x daily. Potent AMPK activator (metformin alternative).
- Magnesium: 300-500mg. Cofactor for signaling.
- Alpha-Lipoic Acid: 300-600mg. Increases GLUT4 translocation.
- Omega-3s: 2-3g EPA/DHA daily.
The goal isn’t “Low Insulin” or “No Carbs”—it is Metabolic Flexibility.
The Hormonal Optimisation Protocol
A 90-day systematic programme to identify, counteract, and permanently reduce cognitive biases in your decision-making — from individual recognition through organisational transformation to permanent integration.
Based on Kahneman, Tetlock, Klein, and 40+ years of decision science research
Day Complete
Great work on your hormonal optimisation practice.
Risks, Limitations &
The Dark Side
This section presents the strongest arguments against aggressive hormonal optimization. It identifies genuine risks, limitations, and scenarios where these protocols may fail or cause harm.
When Optimization Fails
30-50% of baseline hormonal levels are genetically determined. Some individuals have naturally low testosterone, poor thyroid conversion, or insulin resistance despite optimal lifestyle.
- Polymorphisms: CYP19A1 (aromatase), SRD5A2 (5-alpha-reductase), AR sensitivity.
- Family history of metabolic/thyroid disease.
- Ethnic variations in hormone metabolism.
A man genetically predisposed to 400 ng/dL may optimize to 550 ng/dL but never reach 800 ng/dL naturally. Recognize when you've reached your genetic ceiling.
Optimization slows but does not stop aging. Testosterone drops ~1-2% annually after 30; GH declines ~14% per decade.
Optimized: 500-600 ng/dL.
Sedentary: 250-350 ng/dL.
Verdict: Better than peers, but lower than youth.
The first 80% of results comes from 20% of effort (Sleep, Food, Training). The last 5% requires obsessive effort.
Perfectionism creates stress (cortisol) that negates benefits. Accept 85-90% optimization. Perfect hormones don't equal a perfect life.
Genuine Risks of Aggressive Optimization
Excessive volume without recovery chronically elevates cortisol and suppresses testosterone.
Chronic stress → Sustained Cortisol → Suppressed GnRH/LH → Low Testosterone + High SHBG.
Data: Athletes training >15h weekly without recovery show 15-30% lower T than those training 8-12h.
- Monitor HRV daily.
- Schedule deload weeks every 4-6 weeks.
- Ensure caloric sufficiency (Deficit + High Volume = Disaster).
Very low body fat (<2 ng/mL Leptin) signals starvation to the hypothalamus, shutting down reproduction.
- Men <8% Body Fat: Testosterone drops 20-50% despite lean mass.
- Women <15% Body Fat: Amenorrhea and bone density loss.
Bodybuilder at 5% BF training 10+ hours often drops to 250-350 ng/dL. Restoring fat to 8-10% restores levels to 600+ ng/dL.
Aggressive stacks can stress the liver and mask lifestyle deficits.
- Ashwagandha: Rare hepatotoxicity at high doses (>1000mg).
- Green Tea Extract: Hepatotoxicity reported at high doses.
- Prevention: Monitor enzymes (ALT/AST) every 6-12 months. Cycle herbs (8 wks on / 4 off).
Lifestyle cannot fix pathology. Do not attempt to "biohack" the following without medical aid:
- Primary Hypogonadism: Testicular failure requires TRT.
- Hypothyroidism: Hashimoto's requires medication.
- Type 2 Diabetes: Advanced resistance needs Metformin + Lifestyle.
Testosterone <300 ng/dL despite 6 months of optimization. TSH >4.5. Fasting Glucose >100 mg/dL.
The Dark Side: Psychological Risks
1. Orthorexia
Healthy optimization morphs into anxiety-driven perfectionism.
Data: Bodybuilders show 30-50% rates of orthorexia vs 1-7% general population.
Signs: Anxiety when protocols fail, social isolation, self-worth tied to metrics.
2. Nocebo Effects
Knowledge of numbers creates anxiety that worsens function.
Mechanism: See "Low T" result → Anxiety → High Cortisol → Lower T → Vicious Cycle.
Prevention: Do not test if feeling well. Stop tracking if numbers create distress.
Social connection predicts longevity better than biomarkers. If optimization protocols force you to refuse dinner invitations or sacrifice relationships, net quality of life decreases.
- Active Eating Disorder: Fasting/tracking triggers relapse.
- Severe Psychiatric Conditions: Bipolar (manic risk).
- CV Disease: Uncontrolled hypertension/arrhythmias (HIIT/Cold risk).
- Pregnancy/Adolescence: Inappropriate.
- Chronic Kidney Disease: Protein needs adjustment.
- Liver Disease: Supplements contraindicated.
- Autoimmune: Intense training may exacerbate.
- Prior Steroid Use: Natural optimization may be insufficient.
The Bottom Line
"Optimal hormones are a means to a better life, not the goal itself. If optimization reduces your quality of life, you are doing it wrong."
Your Questions Answered
16 research-backed answers covering hormone science, optimization strategies, and common myths — from understanding your endocrine system to protocol implementation.
No questions match your search
Try different keywords or
01Why do hormones matter so much for performance?
Hormones are the operating system on which all performance software runs — you can have perfect training, optimal nutrition, and adequate sleep and still perform at 60% capacity if your endocrine system is suboptimal.
Your hormonal environment determines muscle protein synthesis rate, fat oxidation capacity, cognitive sharpness, emotional resilience, recovery speed, and metabolic efficiency. These aren't independent variables — they're outputs of an integrated signalling network where testosterone, cortisol, growth hormone, thyroid hormones, and insulin constantly interact through feedback loops, synergies, and antagonisms. The mortality link is equally compelling: men with testosterone in the lowest quartile (below 300 ng/dL) have 88% higher cardiovascular mortality compared to the highest quartile. Within the "normal" clinical range, the functional difference between 400 ng/dL and 700 ng/dL is profound — affecting everything from morning energy to training recovery to decision-making quality.
Two executives follow identical training and nutrition programmes. One has a testosterone level of 680 ng/dL with healthy cortisol rhythm; the other sits at 350 ng/dL with flattened cortisol. After 12 weeks, the first has gained 4kg of lean mass and reports sustained mental clarity. The second has gained 1kg, feels chronically fatigued, and is considering quitting the programme. Same inputs, dramatically different hormonal environment.
Hormones amplify or attenuate every other intervention you make. Optimising your endocrine system doesn't replace training and nutrition — it multiplies their returns. **Citations:** 1. Laughlin, G. A. et al. (2008). Low serum testosterone and mortality in older men. *Journal of Clinical Endocrinology & Metabolism*, 93(1), 68–75. 2. Vingren, J. L. et al. (2010). Testosterone physiology in resistance exercise and training. *Sports Medicine*, 40(12), 1037–1053.
02What's the difference between total and free testosterone?
Total testosterone measures all testosterone in your blood, but 60–70% is tightly bound to SHBG (sex hormone binding globulin) and biologically inactive — free testosterone (2–3% of total) is what actually enters cells and drives performance effects.
A man with total testosterone of 500 ng/dL but very high SHBG may have lower functional testosterone than a man at 400 ng/dL with normal SHBG. This distinction is clinically critical because many factors that raise SHBG — aging, certain medications, hyperthyroidism — can mask declining bioavailable testosterone behind an apparently adequate total number. Bioavailable testosterone (free + loosely albumin-bound, approximately 40–50% of total) is the most accurate measure of functional hormone status. SHBG increases with age, chronic stress, and excessive endurance training; it decreases with obesity (initially) and insulin resistance. When evaluating your hormonal status, always request free or bioavailable testosterone alongside total — the total number alone can be profoundly misleading.
A 45-year-old lawyer gets blood work showing total testosterone at 520 ng/dL — "normal" according to his GP. But his SHBG is elevated at 65 nmol/L, leaving free testosterone at just 7.2 pg/mL (bottom 10th percentile). Functionally, he's hypogonadal despite a normal-looking total number. Only when free T is measured does the picture become clear.
Total testosterone is a starting point but never the whole story. Free or bioavailable testosterone tells you what's actually working in your body. Always test both. **Citations:** 1. Vermeulen, A. et al. (1999). A critical evaluation of simple methods for the estimation of free testosterone in serum. *Journal of Clinical Endocrinology & Metabolism*, 84(10), 3666–3672. 2. Antonio, L. et al. (2016). Associations between sex steroids and the development of metabolic syndrome. *Journal of Clinical Endocrinology & Metabolism*, 101(4), 1482–1492.
03Does testosterone really decline with age, and can I prevent it?
Testosterone declines 1–2% annually after age 30 — but this rate is highly modifiable through lifestyle, and fit men in their 60s regularly maintain levels matching sedentary men in their 30s.
The decline is real but variable. Cross-sectional studies show average drops of 110 ng/dL per decade after 30, but the distribution is enormous — some 60-year-olds have levels above 700 ng/dL while some 35-year-olds sit below 300 ng/dL. The modifiable accelerators of decline are: excess body fat (adipose tissue converts testosterone to oestrogen via aromatase), chronic sleep deprivation (70% of daily testosterone is produced during sleep), physical inactivity (resistance training provides acute and chronic testosterone elevation), chronic psychological stress (cortisol directly suppresses GnRH and LH), and environmental endocrine disruptors (xenoestrogens from plastics and chemicals). Addressing all five can increase natural testosterone by 20–40% — often enough to move someone from symptomatic low-T into optimal ranges without medical intervention.
A 52-year-old CEO's bloodwork shows total T at 380 ng/dL (low-normal). Rather than starting TRT, he implements: 4x/week heavy resistance training, sleep optimisation (7.5 hours, cool dark room), 15kg fat loss over 6 months, stress management via daily breathing practice, and elimination of plastic food containers. Re-test at 6 months: 590 ng/dL. No exogenous hormones needed.
Age loads the gun; lifestyle pulls the trigger. A 20–40% natural increase is achievable through systematic lifestyle optimisation before considering medical intervention. **Citations:** 1. Travison, T. G. et al. (2007). A population-level decline in serum testosterone levels in American men. *Journal of Clinical Endocrinology & Metabolism*, 92(1), 196–202. 2. Kumagai, H. et al. (2016). Increased physical activity has a greater effect than reduced energy intake on lifestyle modification-induced increases in testosterone. *Journal of Clinical Biochemistry and Nutrition*, 58(1), 84–89.
04How do hormones interact with each other?
Your hormones exist in dynamic equilibrium — testosterone and cortisol are antagonistic (chronic stress suppresses T by 20–40%), insulin and growth hormone counter-regulate each other, and thyroid hormones set the metabolic rate for the entire system.
The key interactions: Cortisol directly inhibits GnRH and LH production at the hypothalamic-pituitary level, meaning chronic stress biochemically suppresses testosterone synthesis — not through willpower but through measurable hormonal interference. Insulin resistance suppresses testosterone production while simultaneously increasing SHBG binding, creating a double hit to bioavailable T. Growth hormone and insulin are counter-regulatory — GH promotes fat oxidation while insulin promotes storage — which is why GH peaks during fasting and sleep (low insulin states). Thyroid hormones (T3/T4) regulate the metabolic rate for all processes including hormone synthesis, meaning subclinical hypothyroidism silently impairs testosterone, GH, and cognitive function. Leptin signals energy availability to the reproductive axis — excessive leanness (very low body fat) suppresses testosterone as the body deprioritises reproduction.
A CrossFit athlete overtraining 6 days/week with caloric restriction has chronically elevated cortisol, depleted leptin from low body fat, and suppressed thyroid from under-eating. Despite maximal training stimulus, his testosterone drops to 280 ng/dL. The fix isn't more training — it's managing the hormonal web: reducing training volume, increasing calories, improving sleep, and addressing cortisol.
You're not optimising one hormone — you're optimising an interconnected system. Fixing cortisol improves testosterone. Improving insulin sensitivity enhances GH. Restoring thyroid supports everything. Address the network, not individual nodes. **Citations:** 1. Cumming, D. C. et al. (1983). Reproductive hormone increases in response to acute exercise in men. *Medicine and Science in Sports and Exercise*, 15(5), 369–373. 2. Hackney, A. C. (2006). Effects of endurance exercise on the reproductive system of men: the "exercise-hypogonadal male condition." *Journal of Endocrinological Investigation*, 31(10), 932–938.
05What are endocrine disruptors and how much should I worry?
Modern environments contain thousands of synthetic chemicals — xenoestrogens in plastics, anti-androgens in personal care products — that bind to hormone receptors and disrupt endocrine signalling, and reducing exposure alone can increase testosterone by 10–20%.
The two primary threat classes are xenoestrogens (BPA in plastics and thermal receipts, parabens in cosmetics) that mimic oestrogen and bind to hormone receptors, and anti-androgens (phthalates in soft plastics and lotions, certain pesticides) that directly reduce testosterone production. These are not theoretical concerns — population-level testosterone has declined approximately 1% per year since the 1980s beyond what aging alone explains, and environmental chemical exposure is the leading hypothesis. The high-leverage mitigation protocol: use glass or stainless steel for food storage, never microwave plastic, filter drinking water (activated carbon removes most chemicals), avoid thermal receipts, use cast iron or stainless steel cookware, and switch to fragrance-free personal care products. These changes cost little but remove the most significant exposure pathways.
A family switches from plastic food containers to glass, installs a water filter, and eliminates fragranced laundry detergent. The father's urinary BPA levels drop 66% within 3 days. At his next blood test 3 months later, free testosterone has increased 14% — with no other lifestyle changes.
You can't eliminate all exposure, but removing the biggest sources — plastic food contact, unfiltered water, fragranced products — is low-cost, low-effort, and produces measurable hormonal improvement. **Citations:** 1. Gore, A. C. et al. (2015). EDC-2: The Endocrine Society's second scientific statement on endocrine-disrupting chemicals. *Endocrine Reviews*, 36(6), E1–E150. 2. Travison, T. G. et al. (2007). A population-level decline in serum testosterone levels in American men. *Journal of Clinical Endocrinology & Metabolism*, 92(1), 196–202.
06What type of exercise best increases testosterone?
Heavy compound resistance training at 70–85% of your one-rep max produces the strongest acute testosterone response — 15–40% elevation post-session — with chronic adaptations that maintain higher baseline levels over months and years.
The mechanism is mechanical tension: large muscle groups under heavy load (squats, deadlifts, bench press, rows) signal the hypothalamic-pituitary-gonadal axis to upregulate testosterone production. The optimal protocol: 3–4 sessions per week, 30–45 minutes of compound movements, 6–12 rep range, 60–90 second rest periods. Endurance training has the opposite effect when excessive — chronic high-volume cardio (marathon training) elevates cortisol and can suppress testosterone by 20–40%, a condition called "exercise-hypogonadal male condition." Moderate cardio (150 minutes/week) is fine and supports cardiovascular health without endocrine disruption. The key is intensity over volume: shorter, heavier sessions with adequate recovery produce superior hormonal profiles compared to longer, lighter sessions.
A previously sedentary 38-year-old man begins a 3x/week barbell programme (squat, deadlift, overhead press, bench press). After 12 weeks, his total testosterone increases from 420 ng/dL to 560 ng/dL — a 33% increase with no other intervention. His body composition shifts simultaneously: 3kg lean mass gained, 5kg fat lost.
Lift heavy, compound movements, 3–4 times per week, 30–45 minutes. This is the single most powerful natural testosterone intervention available — more effective than any supplement on the market. **Citations:** 1. Kraemer, W. J. & Ratamess, N. A. (2005). Hormonal responses and adaptations to resistance exercise and training. *Sports Medicine*, 35(4), 339–361. 2. Hackney, A. C. et al. (2005). Testosterone responses to intensive interval versus steady-state endurance exercise. *Journal of Endocrinological Investigation*, 28(4), 234–238.
07How does sleep affect testosterone production?
Approximately 70% of daily testosterone is produced during sleep — particularly during REM cycles — and restricting sleep to 5 hours per night for just one week reduces testosterone by 10–15%, equivalent to aging 10–15 years.
Testosterone follows a circadian pattern: levels peak in early morning (which is why morning erections are a crude health marker), dip in the afternoon, and begin rising again during sleep. The production pathway requires pulsatile GnRH release from the hypothalamus, which is heavily modulated by sleep quality and duration. Deep sleep and REM sleep are when the majority of the pulsatile release occurs. Sleep fragmentation — even without reducing total duration — disrupts these pulses and impairs production. Obstructive sleep apnoea, for instance, suppresses testosterone through both fragmentation and hypoxia. The implication is clear: no training programme or nutrition plan can compensate for chronically insufficient sleep. The hormonal factory requires 7–9 hours of quality sleep architecture to run at capacity.
A study at the University of Chicago restricted healthy young men to 5 hours of sleep for one week. Testosterone levels dropped 10–15% — equivalent to aging the participants by a decade. The men also reported decreased vigour, reduced libido, and impaired mood. One week of sleep restriction produced hormonal changes that would take 10–15 years of aging to produce naturally.
Sleep is the single largest determinant of testosterone production. Before adjusting anything else in your protocol, ensure you're getting 7–9 hours of quality sleep with intact architecture. This is non-negotiable. **Citations:** 1. Leproult, R. & Van Cauter, E. (2011). Effect of 1 week of sleep restriction on testosterone levels in young healthy men. *JAMA*, 305(21), 2173–2174. 2. Andersen, M. L. & Tufik, S. (2008). The effects of testosterone on sleep and sleep-disordered breathing in men. *Sleep Medicine Reviews*, 12(5), 365–379.
08Can nutrition significantly move the needle on hormones?
Yes — dietary fat provides the raw material (cholesterol is the precursor for all steroid hormones), protein supplies amino acid building blocks for peptide hormones, and specific micronutrient deficiencies in zinc, magnesium, and vitamin D directly impair endocrine function.
Cholesterol is the molecular backbone of testosterone, cortisol, oestrogen, and all steroid hormones. Very low-fat diets (below 20% of calories) reliably suppress testosterone production because the raw material is insufficient. The optimal range is 25–40% of calories from fat, emphasising monounsaturated (olive oil, avocado) and saturated sources (eggs, red meat, coconut oil) alongside omega-3 fatty acids. Zinc is a direct cofactor in testosterone synthesis — deficiency drops T by up to 50%. Magnesium supports over 300 enzymatic reactions including hormone production. Vitamin D functions as a hormone itself and is strongly correlated with testosterone levels. Caloric deficit is also a hormonal factor: prolonged restriction below maintenance suppresses thyroid, testosterone, and leptin — which is why crash diets destroy hormonal health. Strategic approaches like moderate caloric cycling or time-restricted eating preserve hormonal status while allowing fat loss.
A bodybuilder preparing for competition drops dietary fat to 15% of calories while running a severe caloric deficit for 16 weeks. His testosterone crashes from 650 ng/dL to 180 ng/dL — essentially clinical hypogonadism induced by diet alone. After competition, restoring fat intake to 30% and calories to maintenance, levels recover to 600 ng/dL within 8 weeks.
Eat enough fat (25–40% of calories), adequate protein (1.6–2.2g/kg), and ensure zinc, magnesium, and vitamin D status through food or targeted supplementation. Avoid prolonged severe caloric restriction. **Citations:** 1. Dorgan, J. F. et al. (1996). Effects of dietary fat and fiber on plasma and urine androgens and estrogens in men. *American Journal of Clinical Nutrition*, 64(6), 850–855. 2. Prasad, A. S. et al. (1996). Zinc status and serum testosterone levels of healthy adults. *Nutrition*, 12(5), 344–348.
09Is TRT (testosterone replacement therapy) a good idea?
TRT addresses only one axis while suppressing your natural production — it should be a last resort after 6–12 months of systematic lifestyle optimisation, not a first-line treatment for modifiable low testosterone.
Exogenous testosterone provides the end product but shuts down the HPG axis: the hypothalamus and pituitary stop signalling because external testosterone satisfies the feedback loop. This means natural production ceases, testicular volume decreases, and fertility is typically impaired. Once started, TRT is generally lifelong because restarting natural production is difficult. The legitimate use case: men with genuinely low testosterone (below 300 ng/dL on multiple morning draws) who have optimised sleep, training, nutrition, body composition, and stress management for 6–12 months without adequate improvement. For these men, TRT can be transformative. The problem: many clinics prescribe TRT to men with modifiable lifestyle-driven low T, creating dependency when lifestyle changes would have resolved the issue.
A 40-year-old accountant with T at 320 ng/dL visits a men's health clinic and is offered TRT immediately. Instead, he implements the full optimisation protocol: loses 12kg of body fat, begins 4x/week resistance training, fixes sleep, and reduces alcohol. Six months later, his T is 530 ng/dL — well above the threshold for symptoms — without exogenous hormones, without dependency, and with his natural production pathway intact.
Exhaust lifestyle optimisation first (6–12 months). If genuinely low testosterone persists despite optimal lifestyle, TRT under medical supervision is a reasonable intervention. But most men who "need" TRT actually need a gym membership, sleep hygiene, and body fat reduction. **Citations:** 1. Bhasin, S. et al. (2018). Testosterone therapy in men with hypogonadism. *Journal of Clinical Endocrinology & Metabolism*, 103(5), 1715–1744. 2. Corona, G. et al. (2011). Body weight loss reverts obesity-associated hypogonadotropic hypogonadism. *European Journal of Endocrinology*, 164(5), 801–806.
10Do testosterone "boosters" actually work?
The vast majority of marketed testosterone boosters lack meaningful evidence — the few with robust data (ashwagandha, zinc, vitamin D) primarily work by correcting deficiencies rather than elevating levels above your natural ceiling.
The supplement industry generates billions from testosterone boosters, but systematic reviews consistently find that most products fail to deliver clinically significant testosterone increases. The exceptions with genuine evidence: ashwagandha (KSM-66 standardised extract) has shown 15–17% testosterone increases in stressed men, likely through cortisol reduction rather than direct testosterone stimulation. Zinc supplementation increases testosterone only in men who are zinc-deficient — it corrects a deficiency, not a limitation. Vitamin D supplementation (3,000–5,000 IU daily) is associated with higher testosterone levels, again primarily in those who are deficient. Fenugreek, tribulus, and DHEA have weak or inconsistent evidence. The honest ROI calculation: the money spent on a monthly supplement stack would be better invested in quality protein, a gym membership, and blackout curtains — interventions with dramatically larger effect sizes.
A man spends £120/month on a branded testosterone support stack containing tribulus, fenugreek, D-aspartic acid, and various herbs. After 3 months, his testosterone is unchanged. He redirects that budget to: quality grass-fed beef (zinc, cholesterol), a gym membership, and magnesium glycinate before bed. At 3 months: testosterone up 22%. The boring basics outperformed the exotic stack.
Test for deficiencies (zinc, vitamin D, magnesium) and correct them. Consider ashwagandha if you're chronically stressed. Skip everything else and invest in training, sleep, and nutrition — the proven interventions that actually move the needle. **Citations:** 1. Lopresti, A. L. et al. (2019). A randomized, double-blind, placebo-controlled, crossover study examining the hormonal and vitality effects of ashwagandha in aging, overweight males. *American Journal of Men's Health*, 13(2), 1557988319835985. 2. Clements, A. et al. (2021). Testosterone boosters intake in athletes: current evidence and further directions. *Sexual Medicine Reviews*, 9(4), 636–651.
11How does cortisol dysregulation affect my performance?
The problem isn't cortisol itself — it's a disrupted rhythm. Healthy cortisol features a sharp morning spike for alertness and a gradual decline to near-zero by evening. Chronic stress flattens this curve, leaving you wired at night and exhausted in the morning.
Acute cortisol elevation is adaptive and essential — it mobilises energy, sharpens focus, and powers through challenges. Elite performers actually produce higher acute cortisol spikes than average but recover faster, maintaining the sharp peak-and-valley rhythm. The pathology is chronic elevation or a flattened diurnal pattern where cortisol never fully drops. This creates a cascade: suppressed testosterone production (cortisol directly inhibits GnRH), impaired insulin sensitivity, disrupted sleep architecture (elevated evening cortisol prevents sleep onset), hippocampal atrophy (memory impairment), and increased visceral fat deposition. Burnout risk is 3–5x higher with cortisol dysregulation. The diagnostic indicators: difficulty waking despite adequate hours (blunted morning cortisol), second wind of energy at 10pm (elevated evening cortisol), poor recovery between training sessions, and persistent abdominal fat despite caloric control.
A startup founder running on caffeine and adrenaline has a cortisol profile that's essentially flat — moderate all day, moderate all night. She's simultaneously fatigued and wired. After 8 weeks of morning light exposure, evening screen restriction, daily breathing practice, and training volume reduction, her cortisol curve resharpens: high morning peak, low evening trough. Sleep quality improves, testosterone rises, and she describes feeling "like a different person."
Cortisol isn't the enemy — a broken cortisol rhythm is. Restore the healthy peak-and-valley pattern through circadian alignment, stress management, and training periodisation. **Citations:** 1. Adam, E. K. et al. (2017). Diurnal cortisol slopes and mental and physical health outcomes: a systematic review and meta-analysis. *Psychoneuroendocrinology*, 83, 25–41. 2. Tsigos, C. & Chrousos, G. P. (2002). Hypothalamic-pituitary-adrenal axis, neuroendocrine factors and stress. *Journal of Psychosomatic Research*, 53(4), 865–871.
12What role does thyroid health play in performance?
Thyroid hormones (T3 and T4) set the metabolic rate for your entire body — including brain metabolism, hormone synthesis, and energy production — making subclinical hypothyroidism a silent performance killer that reduces testosterone, GH, and cognitive function simultaneously.
The thyroid is the metabolic thermostat. When T3 (the active form) is low, everything slows: mitochondrial energy production drops, neurotransmitter synthesis decreases, body temperature falls, and other hormone production is impaired. Subclinical hypothyroidism (TSH elevated but T3/T4 still within "normal" range) is extremely common and frequently missed on standard blood panels that only test TSH. Symptoms overlap with burnout and depression: fatigue, brain fog, weight gain, cold sensitivity, dry skin, and low motivation. The modifiable factors: selenium deficiency impairs T4-to-T3 conversion, chronic stress suppresses thyroid function via the HPA axis, excessive endurance training can reduce T3, and severe caloric restriction downregulates thyroid output as an energy-conservation mechanism. A comprehensive thyroid panel (TSH, free T3, free T4, reverse T3, TPO antibodies) is essential for anyone experiencing persistent fatigue despite adequate sleep.
A triathlete training 15+ hours per week on a moderate caloric deficit has persistent fatigue, difficulty recovering, and declining performance despite increasing training volume. Blood work reveals free T3 at the bottom of the reference range with elevated reverse T3 — his body is downregulating thyroid function to conserve energy. Reducing training volume to 10 hours and increasing calories by 400/day normalises thyroid function within 6 weeks, and paradoxically, his race times improve.
If you're doing everything right and still feel flat, get a comprehensive thyroid panel — not just TSH. Thyroid dysfunction is one of the most common and most overlooked causes of persistent fatigue in high performers. **Citations:** 1. Biondi, B. & Cooper, D. S. (2008). The clinical significance of subclinical thyroid dysfunction. *Endocrine Reviews*, 29(1), 76–131. 2. Hackney, A. C. & Aggon, E. (2018). Chronic low testosterone levels in endurance trained men: the exercise-hypogonadal male condition. *Journal of Biochemistry and Physiology*, 1(1), 103.
13How do I maximise natural growth hormone production?
Growth hormone peaks during deep sleep and in low-insulin states — the two most powerful natural stimuli are quality sleep architecture and intermittent fasting, which can produce GH surges of 300–500% above baseline.
GH is fundamentally counter-regulatory to insulin: it promotes fat oxidation and tissue repair while insulin promotes storage. This means GH peaks when insulin is low — during sleep (particularly the first deep sleep cycle) and during fasting states. Heavy resistance training produces acute GH spikes, especially with shorter rest periods (60–90 seconds) and higher metabolic stress. Fasted training in the morning combines the overnight fast with exercise stimulus for maximal GH response. Intermittent fasting (12–16 hour overnight fast, 3–5 days weekly) maintains the low-insulin window that permits GH release. GH declines approximately 14% per decade after 30, but this rate is modifiable through the same lifestyle factors: sleep quality, training intensity, and metabolic health. The age-related decline is largely driven by loss of deep sleep, increased body fat, and reduced training intensity — all addressable.
A 48-year-old implements a simple protocol: heavy squats and deadlifts 3x/week, 16:8 intermittent fasting on training days (fasted morning training, feeding window 12–8pm), and sleep optimisation targeting deep sleep. His body composition shifts from 25% to 18% body fat over 4 months, consistent with enhanced GH-driven fat oxidation and protein synthesis — without any exogenous hormones.
Protect deep sleep, train heavy in a fasted state when possible, and use intermittent fasting to maintain low-insulin windows. These three strategies maximise your body's natural GH production at any age. **Citations:** 1. Ho, K. Y. et al. (1988). Fasting enhances growth hormone secretion and amplifies the complex rhythms of growth hormone secretion in man. *Journal of Clinical Investigation*, 81(4), 968–975. 2. Godfrey, R. J. et al. (2003). The exercise-induced growth hormone response in athletes. *Sports Medicine*, 33(8), 599–613.
14Why is insulin sensitivity so important beyond diabetes?
Insulin sensitivity determines how efficiently your body partitions nutrients — high sensitivity means glucose goes to muscle and brain; low sensitivity (insulin resistance) means excess storage as fat, chronic inflammation, and direct suppression of testosterone and growth hormone.
Insulin isn't just about blood sugar — it's a master regulator that interacts with every other hormonal axis. Hyperinsulinaemia (chronic elevated insulin from resistance) suppresses SHBG, reduces free testosterone bioavailability, blunts growth hormone release, increases cortisol, and drives visceral fat accumulation — which itself produces more aromatase (converting testosterone to oestrogen). This creates a vicious cycle: insulin resistance → lower testosterone → more visceral fat → more insulin resistance. The positive cycle is equally powerful: improving insulin sensitivity through resistance training, time-restricted eating, and reducing refined carbohydrates creates cascading improvements across all hormonal axes simultaneously. Post-exercise insulin sensitivity is 3–5x higher than baseline, which is why strategic carbohydrate timing (30–50% of daily carbs consumed post-training) leverages this window for maximum nutrient partitioning.
A sedentary manager with insulin resistance and testosterone at 340 ng/dL begins resistance training 4x/week and shifts to a 10-hour eating window with carbs concentrated post-workout. After 4 months, his fasting insulin drops 40%, body fat drops from 28% to 22%, and testosterone rises to 510 ng/dL. He didn't "boost" testosterone — he removed the metabolic brake that was suppressing it.
Insulin sensitivity is the metabolic foundation that all other hormonal optimisation depends on. Fix insulin sensitivity through training, nutrition timing, and body composition — and watch every other hormone improve as a downstream effect. **Citations:** 1. Pitteloud, N. et al. (2005). Increasing insulin resistance is associated with a decrease in Leydig cell testosterone secretion in men. *Journal of Clinical Endocrinology & Metabolism*, 90(5), 2636–2641. 2. Ivy, J. L. (2004). Regulation of muscle glycogen repletion, muscle protein synthesis and repair following exercise. *Journal of Sports Science and Medicine*, 3(3), 131–138.
15What blood tests should I get before starting a hormonal optimisation protocol?
At minimum: total testosterone, free testosterone, SHBG, oestradiol, cortisol (morning), full thyroid panel (TSH, free T3, free T4, reverse T3), fasting insulin, fasting glucose, HbA1c, vitamin D, zinc, and magnesium RBC — tested via a morning fasted blood draw before 10am.
Timing matters enormously for hormonal blood work. Testosterone peaks between 7–10am and can be 30% lower by afternoon, so always test fasted before 10am for accurate results. A single low reading isn't diagnostic — retest to confirm before making any protocol decisions. The comprehensive panel provides a systems view: testosterone and SHBG reveal androgenic status, oestradiol shows aromatisation rate (important for men with excess body fat), morning cortisol indicates adrenal function, the thyroid panel identifies subclinical dysfunction, and metabolic markers (insulin, glucose, HbA1c) reveal insulin resistance that may be suppressing the entire endocrine system. Vitamin D, zinc, and magnesium are the most common cofactor deficiencies that impair hormone production. Cost-effective approach: use a direct-to-consumer lab service (Medichecks, Forth, or similar) for baseline testing, then retest at 3 and 6 months to track intervention effects.
A 36-year-old runner gets a baseline panel revealing: total T 480 ng/dL (adequate), but free T low at 8.1 pg/mL (high SHBG), vitamin D deficient at 22 ng/mL, zinc borderline, and fasting insulin elevated at 14 mIU/L. The interventions are now precision-targeted: vitamin D and zinc supplementation, insulin sensitivity work through resistance training and dietary changes, and investigation of why SHBG is elevated.
Test before you optimise — you can't improve what you haven't measured. Morning fasted blood draw, comprehensive panel, retest at 3 and 6 months to confirm your interventions are working. **Citations:** 1. Bhasin, S. et al. (2010). Testosterone therapy in men with androgen deficiency syndromes. *Journal of Clinical Endocrinology & Metabolism*, 95(6), 2536–2559. 2. Crawford, E. D. et al. (2007). The importance of serial measurements in the early detection of testosterone deficiency. *Therapeutic Advances in Urology*, 7(4), 239–245.
16What's the optimal order for implementing a hormonal optimisation protocol?
Start with sleep and stress management (weeks 1–2), then add resistance training and nutritional foundations (weeks 3–4), then address environment and supplementation (weeks 5–8), and only consider medical intervention after 6–12 months of optimised lifestyle.
The sequence matters because each layer amplifies the next. Sleep optimisation (7–9 hours, cool dark room, consistent wake time) is first because 70% of testosterone is produced during sleep — no other intervention works at full capacity on broken sleep. Stress management (breathing practice, training volume control, workload boundaries) is paired with sleep because cortisol dysregulation suppresses the entire HPG axis. Resistance training (compound movements, progressive overload, 3–4x weekly) provides the strongest natural testosterone stimulus but requires adequate sleep and stress management to produce results without overtraining. Nutritional foundations (adequate fat, protein, micronutrients) ensure the raw materials are available for hormone synthesis. Environmental detox (reducing endocrine disruptors) and targeted supplementation (vitamin D, zinc, magnesium) provide the final optimisation layer. This progressive approach prevents overwhelm, builds sustainable habits, and produces measurable improvements at each stage.
Month 1: Fix sleep (consistent 7am wake, cool dark room, no screens 90 min before bed) + daily box breathing. Month 2: Add 3x/week barbell training + optimise protein and fat intake. Month 3: Switch to glass food storage, add vitamin D/zinc/magnesium, begin intermittent fasting 2x/week. Retest blood work at month 3 and month 6. Most men see 20–40% testosterone improvement by month 6 with this systematic approach.
Sleep → Stress → Training → Nutrition → Environment → Supplements → Medical (if needed). Each layer builds on the last. Skipping to supplements or TRT without fixing sleep and stress is building on a cracked foundation. **Citations:** 1. Kumagai, H. et al. (2016). Increased physical activity has a greater effect than reduced energy intake on lifestyle modification-induced increases in testosterone. *Journal of Clinical Biochemistry and Nutrition*, 58(1), 84–89. 2. Leproult, R. & Van Cauter, E. (2011). Effect of 1 week of sleep restriction on testosterone levels in young healthy men. *JAMA*, 305(21), 2173–2174.
You've explored all 16 questions
Ready to go deeper? The full Hormonal Optimization article provides comprehensive frameworks, implementation protocols, and advanced optimization systems.
Your Hormonal
Optimization Journey
You now possess a comprehensive, science-based framework for systematically optimizing your endocrine system—the master control network governing strength, body composition, cognitive performance, energy, mood, and longevity.
The Core Principles Revisited
1. Integration, Not Isolation
Hormones are integrated. Optimizing testosterone while ignoring cortisol dysregulation fails. Comprehensive optimization requires systems thinking: sleep, training, nutrition, and stress management all interact.
2. Lifestyle is the Engine
Lifestyle factors produce 70-80% of results. Sleep (7-9h), Training (3-4x/week), and Nutrition (Protein/Fats) are the foundations. Supplements are merely marginal gains.
3. Spectrum, Not Binary
Perfect adherence isn't required. Implementing 70-80% of these protocols produces 90% of results. Obsessive perfectionism creates stress that negates benefits.
4. Individual Variation
Genetics, age, and history affect response. Some are high responders; others moderate. Use protocols as frameworks, not rigid prescriptions.
The Hierarchy of Interventions
Sleep 7-9 hours nightly with consistent timing. This single intervention protects testosterone, growth hormone, cortisol rhythm, insulin sensitivity, and thyroid function.
Add Resistance Training (3x weekly) and Nutrient-Dense Nutrition (adequate protein, healthy fats, strategic carbs). This covers the majority of hormonal benefit.
Follow the Basic 30-Day Protocol, then the Advanced Protocol. Monitor subjective well-being and biomarkers. Adjust based on results.
Measuring Success
- Energy levels throughout the day
- Sleep quality and morning alertness
- Training performance and recovery
- Libido and sexual function
- Mood, motivation, and mental clarity
- Blood Work: T/Free T, Cortisol, Insulin, HbA1c, Thyroid.
- Body Comp: Waist circumference, body fat %.
- Performance: Strength gains, endurance.
- HRV: Daily average trends.
"Optimize for how you feel and perform, not just numbers."
Lifestyle optimization is powerful but not a substitute for medical treatment when pathology exists. Consult a specialist if:
- Testosterone: <300 ng/dL despite 12+ weeks optimization.
- Symptoms: Persistent severe fatigue, complete loss of libido, ED, depression.
- Thyroid: TSH >4.5 or symptomatic hypothyroidism.
- Metabolic: Fasting glucose >100 mg/dL or HbA1c >5.7%.
- Conditions: Suspected PCOS, Cushing's, Addison's, or Pituitary disorders.
The Long Game
Hormonal optimization isn't a 30-day challenge. It's a sustainable lifestyle that compounds benefits over decades.
In Your 30s
Prevents age-related decline, maintains performance, establishes habits.
In Your 40s-50s
Slows biological aging, maintains lean mass and metabolic health.
In Your 60s+
Preserves independence, prevents frailty, maintains quality of life and healthspan.
Don't get paralyzed by information overload. Start simple.
- Set consistent sleep/wake schedule.
- Schedule 3 resistance sessions.
- Eliminate one major source of processed sugar.
- Implement Basic 30-Day Protocol.
- Track sleep & subjective well-being.
- Establish non-negotiable habits.
- Get baseline blood work.
- Progress to Advanced Protocol if results are good.
- Refine protocols based on response.
- Establish optimization as lifestyle.
- Retest blood work every 3-6 months.
- Build sustainable practices.
"Master your hormones, and you master your biology. Master your biology, and you unlock your full human potential."
Begin Now.
“All things are poison, and nothing is without poison; the dosage alone makes it so a thing is not a poison.” — Paracelsus
What You Need to Remember
What the research says — stripped of marketing, fear, and bro-science.
Hormones carry instructions, not magic
Hormones are information molecules coordinating behavior across organs. Optimizing them means fixing the signal environment — sleep, stress, nutrition — not chasing isolated numbers on a blood panel.
Explore: Module 1 — Endocrine Logic →The cortisol curve predicts your day
High morning cortisol (alertness), gradual decline, low evening cortisol (sleep prep) — this diurnal pattern predicts cognitive performance, immune function, and recovery better than any single hormone level.
Explore: Module 1 — HPA Dynamics →Sleep drives every hormone that matters
Growth hormone pulses during deep sleep. Testosterone peaks during REM. Melatonin gates recovery. Cortisol resets overnight. No supplement, no training protocol, no lifestyle hack compensates for broken sleep.
Explore: Module 2 — Sleep-Hormone Link →Endocrine disruptors accumulate silently
BPA, phthalates, parabens, and pesticide residues mimic or block hormonal signals at parts-per-billion concentrations. Single exposures are trivial. Decades of daily exposure are not.
Explore: Module 3 — Disruptor Map →Lifestyle changes rival low-dose TRT
Resistance training, sleep optimization, stress reduction, and achieving 15-18% body fat produce testosterone increases of 20-40% — comparable to low-dose replacement therapy, without the side effects or dependency.
Explore: Module 3 — Lifestyle vs Pharma →One blood test doesn't mean anything
Testosterone varies 30-40% within a single day and across seasons. The supplement industry turns one low morning reading into a diagnosis and a recurring subscription. Demand serial testing.
Explore: Module 4 — Diagnostic Literacy →Squat, deadlift, press — the hormonal trifecta
Heavy compound lifts trigger the largest acute hormonal response (testosterone, GH, IGF-1) and the strongest chronic adaptations of any exercise modality. Machines and isolation work don't compare.
Explore: Module 4 — Training Protocol →Cortisol isn't the enemy — flat cortisol is
You need cortisol to focus, to wake up, to mount an immune response. The problem isn't cortisol itself — it's the flattened, chronically elevated pattern that sustained stress creates.
Explore: Module 4 — Cortisol Literacy →Test at the same time, under the same conditions
Total/free testosterone, SHBG, cortisol, thyroid panel, DHEA-S — all fluctuate with time of day, recent sleep, training load, and stress. A number without context is noise, not data.
Explore: Module 5 — Testing Protocol →Lifestyle first. Supplements last. Always.
Sleep, heavy resistance training, stress management, 15-18% body fat, and reduced toxin exposure. Do these first. Then — and only then — consider targeted supplementation for remaining gaps.
Explore: Module 5 — The Integrated Approach →Continue Your Journey
References
0 sources cited — journal articles and landmark studies in testosterone optimization, cortisol management, thyroid function, growth hormone signaling, and insulin sensitivity
- 1(2016). Increased physical activity has a greater effect than reduced energy intake on lifestyle modification-induced increases in testosterone. Journal of Clinical Biochemistry and Nutrition, 58(1), 84–89.
- 2(2011). Effect of 1 week of sleep restriction on testosterone levels in young healthy men. JAMA, 305(21), 2173–2174.
- 3(2017). A perspective on middle-aged and older men with functional hypogonadism: Focus on holistic management. Journal of Clinical Endocrinology & Metabolism, 102(3), 1067–1075.
- 4(2011). Hypogonadism as a risk factor for cardiovascular mortality in men: A meta-analytic study. European Journal of Endocrinology, 165(5), 687–701.
- 5(2007). A population-level decline in serum testosterone levels in American men. Journal of Clinical Endocrinology & Metabolism, 92(1), 196–202.
- 6(2005). Hormonal responses and adaptations to resistance exercise and training. Sports Medicine, 35(4), 339–361.
- 7(2004). Frequent occurrence of hypogonadotropic hypogonadism in type 2 diabetes. Journal of Clinical Endocrinology & Metabolism, 89(11), 5462–5468.
- 8(2011). Low testosterone in men with type 2 diabetes: Significance and treatment. Journal of Clinical Endocrinology & Metabolism, 96(8), 2341–2353.
- 9(2010). The impact of body mass index on semen parameters and reproductive hormones in human males. Human Reproduction Update, 16(3), 293–311.
- 10(2011). Effect of vitamin D supplementation on testosterone levels in men. Hormone and Metabolic Research, 43(3), 223–225.
- 11(1996). Zinc status and serum testosterone levels of healthy adults. Nutrition, 12(5), 344–348.
- 12(2011). Effects of magnesium supplementation on testosterone levels of athletes and sedentary subjects at rest and after exhaustion. Biological Trace Element Research, 140(1), 18–23.
- 13(2010). The cortisol awakening response: More than a measure of HPA axis function. Neuroscience & Biobehavioral Reviews, 35(1), 97–103.
- 14(2014). Effects of stress on immune function: The good, the bad, and the beautiful. Immunologic Research, 58(2-3), 193–210.
- 15(2017). Diurnal cortisol slopes and mental and physical health outcomes: A systematic review and meta-analysis. Psychoneuroendocrinology, 83, 25–41.
- 16(2007). Physiology and neurobiology of stress and adaptation: Central role of the brain. Physiological Reviews, 87(3), 873–904.
- 17(1999). Impact of sleep debt on metabolic and endocrine function. The Lancet, 354(9188), 1435–1439.
- 18(2003). Acute and chronic effects of exercise on tissue sensitivity to glucocorticoids. Journal of Applied Physiology, 94(3), 869–875.
- 19(2006). Chronic stress at work and the metabolic syndrome: Prospective study. BMJ, 332(7540), 521–525.
- 20(2012). A prospective, randomized double-blind, placebo-controlled study of safety and efficacy of a high-concentration full-spectrum extract of Ashwagandha root in reducing stress and anxiety in adults. Indian Journal of Psychological Medicine, 34(3), 255–262.
- 21(1998). The efficacy of Ginkgo biloba on cognitive function in Alzheimer disease. Archives of Neurology, 55(11), 1409–1415.
- 22(2014). Thyroid hormone regulation of metabolism. Physiological Reviews, 94(2), 355–382.
- 23(2002). Biochemistry, cellular and molecular biology, and physiological roles of the iodothyronine selenodeiodinases. Endocrine Reviews, 23(1), 38–89.
- 24(2012). Thyroid function and obesity. European Thyroid Journal, 1(3), 159–167.
- 25(2019). An investigation into the stress-relieving and pharmacological actions of an ashwagandha (Withania somnifera) extract. Medicine, 98(37), e17186.
- 26(2015). Iodine deficiency and thyroid disorders. Lancet Diabetes & Endocrinology, 3(4), 286–295.
- 27(2017). Selenium and thyroid disease: From pathophysiology to treatment. International Journal of Endocrinology, 2017, 1297658.
- 28(2015). Selenium: An element for life. Endocrine, 48(3), 756–775.
- 29(2009). Effects of growth hormone on glucose, lipid, and protein metabolism in human subjects. Endocrine Reviews, 30(2), 152–177.
- 30(1992). Endurance training amplifies the pulsatile release of growth hormone: Effects of training intensity. Journal of Applied Physiology, 72(6), 2188–2196.
- 31(1988). Fasting enhances growth hormone secretion and amplifies the complex rhythms of growth hormone secretion in man. Journal of Clinical Investigation, 81(4), 968–975.
- 32(1998). Interrelations between sleep and the somatotropic axis. Sleep, 21(6), 553–566.
- 33(1992). Augmented growth hormone (GH) secretory burst frequency and amplitude mediate enhanced GH secretion during a two-day fast in normal men. Journal of Clinical Endocrinology & Metabolism, 74(4), 757–765.
- 34(2003). The exercise-induced growth hormone response in athletes. Sports Medicine, 33(8), 599–613.
- 35(2013). Somatotropic signaling: Trade-offs between growth, reproductive development, and longevity. Physiological Reviews, 93(2), 571–598.
- 36(2009). Skeletal muscle insulin resistance is the primary defect in type 2 diabetes. Diabetes Care, 32(Suppl 2), S157–S163.
- 37(2005). Exercise-induced increase in muscle insulin sensitivity. Journal of Applied Physiology, 99(1), 338–343.
- 38(2017). Update on the effects of physical activity on insulin sensitivity in humans. BMJ Open Sport & Exercise Medicine, 2(1), e000143.
- 39(2008). Efficacy of berberine in patients with type 2 diabetes mellitus. Metabolism, 57(5), 712–717.
- 40(2000). Longitudinal compensation for fat-induced insulin resistance includes reduced insulin clearance and enhanced beta-cell response. Diabetes, 49(12), 2116–2125.
- 41(2004). Impaired mitochondrial activity in the insulin-resistant offspring of patients with type 2 diabetes. New England Journal of Medicine, 350(7), 664–671.
- 42(2004). The metabolic syndrome and inflammation. Metabolic Syndrome and Related Disorders, 2(2), 82–104.
- 43(2004). Vinegar improves insulin sensitivity to a high-carbohydrate meal in subjects with insulin resistance or type 2 diabetes. Diabetes Care, 27(1), 281–282.
- 44(2003). Cinnamon improves glucose and lipids of people with type 2 diabetes. Diabetes Care, 26(12), 3215–3218.
- 45(2008). Metabolic consequences of sleep and sleep loss. Sleep Medicine, 9(Suppl 1), S23–S28.
- 46(2009). Sleep curtailment is accompanied by increased intake of calories from snacks. American Journal of Clinical Nutrition, 89(1), 126–133.
- 47(2001). Disruption of the nocturnal testosterone rhythm by sleep fragmentation in normal men. Journal of Clinical Endocrinology & Metabolism, 86(3), 1134–1139.
- 48(2004). Short sleep duration is associated with reduced leptin, elevated ghrelin, and increased body mass index. PLoS Medicine, 1(3), e62.
- 49(2007). The metabolic consequences of sleep deprivation. Sleep Medicine Reviews, 11(3), 163–178.
- 50(1997). Testosterone and cortisol in relationship to dietary nutrients and resistance exercise. Journal of Applied Physiology, 82(1), 49–54.
- 51(1996). Effects of dietary fat and fiber on plasma and urine androgens and estrogens in men: A controlled feeding study. American Journal of Clinical Nutrition, 64(6), 850–855.
- 52(1984). Diet and serum sex hormones in healthy men. Journal of Steroid Biochemistry, 20(1), 459–464.
- 53(2010). Influence of dietary carbohydrate intake on the free testosterone: Cortisol ratio responses to short-term intensive exercise training. European Journal of Applied Physiology, 108(6), 1125–1131.
- 54(1988). Effect of massive weight loss on hypothalamic-pituitary-gonadal function in obese men. Journal of Clinical Endocrinology & Metabolism, 66(5), 1019–1023.
- 55(2008). Letrozole once a week normalizes serum testosterone in obesity-related male hypogonadism. European Journal of Endocrinology, 158(5), 741–747.
- 56(1997). Body fat distribution, the menopause transition, and hormone replacement therapy. Diabetes & Metabolism, 26(1), 12–20.
- 57(2011). Relationship between urinary phthalate and bisphenol A concentrations and serum thyroid measures in U.S. adults and adolescents. Environmental Health Perspectives, 119(10), 1396–1402.
- 58(2005). Decrease in anogenital distance among male infants with prenatal phthalate exposure. Environmental Health Perspectives, 113(8), 1056–1061.
- 59(2009). Endocrine-disrupting chemicals: An Endocrine Society scientific statement. Endocrine Reviews, 30(4), 293–342.
- 60(2013). Bisphenol A and human health: A review of the literature. Reproductive Toxicology, 42, 132–155.
- 61(2015). Examining the effect of Withania somnifera supplementation on muscle strength and recovery. Journal of the International Society of Sports Nutrition, 12(1), 43.
- 62(2013). Effect of Tongkat Ali on stress hormones and psychological mood state in moderately stressed subjects. Journal of the International Society of Sports Nutrition, 10(1), 28.
- 63(2010). Effects of methoxyisoflavone, ecdysterone, and sulfo-polysaccharide supplementation on training adaptations. International Journal of Sport Nutrition and Exercise Metabolism, 20(6), 457–465.
- 64(2011). Coenzyme Q10 improves seminal oxidative defense but does not affect on semen parameters in idiopathic oligoasthenoteratozoospermia. Andrologia, 43(6), 426–431.
- 65(2014). Effect of Coenzyme Q10 supplementation on antioxidant enzymes activity and oxidative stress of seminal plasma. Journal of Endocrinological Investigation, 37(4), 303–308.
- 66(1998). The effects of short-term resistance training on endocrine function in men and women. European Journal of Applied Physiology, 78(1), 69–76.
- 67(2008). Twenty-four-hour cortisol response to multiple daily exercise sessions of moderate and high intensity. Clinical Physiology and Functional Imaging, 19(2), 178–182.
- 68(2003). Basal testicular testosterone production in endurance-trained men is suppressed. European Journal of Applied Physiology, 89(2), 198–201.
- 69(2017). Hormonal aspects of overtraining syndrome: A systematic review. BMC Sports Science, Medicine and Rehabilitation, 9(1), 14.
- 70(2010). Psychophysiological biomarkers of workplace stressors. Neuroscience & Biobehavioral Reviews, 35(1), 51–57.
- 71(2000). Stress and body shape: Stress-induced cortisol secretion is consistently greater among women with central fat. Psychosomatic Medicine, 62(5), 623–632.
- 72(2018). Effects of stress on the development and progression of cardiovascular disease. Nature Reviews Cardiology, 15(4), 215–229.
- 73(2019). An investigation into the stress-relieving and pharmacological actions of an ashwagandha (Withania somnifera) extract: A randomized, double-blind, placebo-controlled study. Medicine, 98(37), e17186.